Lubnin A.Yu., Gromova V.V. Abstract In the work, on the basis of literature data and personal experience, the current state of the problem of blood reinfusion in surgery is analyzed. Technical solutions, methodological approaches, equipment for blood reinfusion in surgical patients are considered. Also considered are such aspects of the problem as indications, contraindications and features of the application of the technique in various areas of surgery.
Reinfusion of blood in surgery. The current state of the problem
For correspondence: Andrey Yurievich Lubnin — Dr. med. Sci., Professor, Head of the Department of Anesthesiology, Resuscitation and Intensive Care of the Federal State Autonomous Institution “N.N. acad. N.N. Burdenko, Ministry of Health of the Russian Federation, Moscow; e-mail: [email protected]
For citation: Lubnin A.Yu., Gromova V.V. Reinfusion of blood in surgery. The current state of the problem. Bulletin of Intensive Care named after A.I. Saltanov. 2019;4:58–67. DOI: 10.21320/1818-474X-2019-4-58-67
In this paper, based on literature data and our own experience, the current state of the problem of blood reinfusion in surgery is analyzed. Technical solutions, methodological approaches, equipment for blood reinfusion in surgical patients are considered. Also considered are such aspects of the problem as indications, contraindications and features of the application of the technique in various areas of surgery.
Keywords: blood reinfusion in surgery, technical solutions, indications and contraindications, possible complications
Received: 06.03.2019
Accepted to printing: 05.11.2019
Introduction
Since the emergence of surgery as a medical discipline to the present day, surgical blood loss, especially massive and rapid, remains one of the most formidable complications of the perioperative period, responsible for insufficient radicalization, disability, and even death. Over the years, humanity has nevertheless learned in a certain way to deal with the problem of surgical blood loss using three main approaches: 1) the use of infusion solutions; 2) transfusions of pre-prepared donor blood components; 3) return to the patient of his own blood, poured out during the operation. All three approaches have a long and rather interesting history, which it is not possible to dwell on in the framework of this short work, but there are interesting publications on this topic, and the interested reader can familiarize themselves with them [1–4]. We only note that all these three approaches are currently being developed and successfully used clinically. Infusion solutions, especially colloidal solutions, allow you to quickly and effectively eliminate the BCC deficiency caused by surgical blood loss, although without replacing the oxygen transport function of lost red blood cells, however, with a volume of up to 30 or 50% of the BCC, this allows you to solve the problem at least for a while.The billet and storage of donor blood components are increasingly improved, but the main problem of this approach associated with the possible infection of the patient remains almost unresolved. Moreover, the year of the year the number of potential infectments transmitted transfusion, expands (viruses, bacteria, simplest, prions, etc. The list is obviously not completed). Perhaps, therefore, the third approach in the form of reinfusion of the patient's own blood, lost during the operation, and sometimes in the near postoperative period, it seems more interesting and promising.
It so happened that six years ago we managed to collect a wonderful author's team – a group of authors from different clinics – and to issue a book on this topic [5]. As far as I know, neither I myself nor other authors of this book have attached any heroic efforts to spread it. Nevertheless, she quickly went around the country and received even certain positive evaluations. Thank you. However, since 2013, six years have passed – the term is not big, but not small, and partly on certain external reasons, partly from the inner motivation, we wanted to see what has changed during this time in clinical "reinfusiology". By contacting the search system PubMed on the topic "Blood Reinfusion", we found more than 2000 publications that are not at all. In addition, in the spring of 2018, I [A.L.] managed to participate in the next NATA session, at which the problem of blood reinfusion was also in the spotlight. Let's try to look at all this carefully.
Terminology
In our opinion, it is important from the very beginning to negotiate the use of adequate terminology. The fact is that at present there are a number of different healing technologies, during the implementation of which the patient's own blood is exfused from its body, followed by a refund. This is primarily a preoperative outdoority (pad) and acute isoovolemic hemodilution (ILGD). It seems to us that these are quite effective independent techniques, but to date them to the reinfusion of blood (RK) is incorrect. Hereinafter, in the presentation, we understand the PCC only the return of blood components derived from its own, lost during surgery.
Easy and hardware reinfusion of blood
This, it would seem that the reader should understand the obvious moment immediately, although the information on this topic in recent years has not changed significantly. It should be immediately noted that the so-called simple (not hardware) methods of the Republic of Kazakhstan currently have more historical significance and can be used clinically only in emergency situations and only to save the life of the patient (the situation of massive internal bleeding, both with impaired ectopic pregnancy; in the absence Available donor blood resource).This is a strict limitation due to the high risk of secondary complications of such an RK, up to the possibility of fatal outcome. Therefore, at present, the use of simple methods of the Republic of Kazakhstan in planned surgical interventions is considered unacceptable [6]. That is, the persistence of some manufacturers looks like, which still continues to produce and trade with simple devices for the Republic of Kazakhstan (Solcotrans Auto, Bellovac ABT Sangvia, and similar to them), which are not providing for any processing of amusing or drainage blood, except for simple filtration.
Powerful wound blood can be somewhat different in its composition in various areas of surgery (for example, an admixture of fat globul in traumatology and orthopedics, amniotic fluid in obstetrics), but in general it is characterized by a high content of such extremely unwanted components, as destroyed erythrocytes and free hemoglobin, activated Leukocytes and platelets and, of course, a large number of different biologically active substances. One of the leading specialists in the world in the Republic of Kazakhstan in Surgery, Professor E. Hanzen generally called such a "soup". It is not surprising that intravenous administration of such a transfusion medium often causes severe consequences [6]. The treatment of wound blood in a selle-sewer by repeated laundering with sterile crystalloid solutions and the subsequent separation in the centrifuge chamber allows, on the one hand, remove all unwanted impurities indicated above, on the other – to obtain the most secure component (caroid autoeritrocytes) [7]. The price of this safety is an irrevocable loss with a flushing fluid platelet and plasma hemostasis factors. But, as clinical practice shows, the question of targeted compensation of such losses becomes relevant only with massive and supermassive blood loss.
Modern Selll Seiversami
For those who have passed from the release of our book for six years, the situation with commercially available selle-seivers has not changed much [8-10]. The same manufacturers and almost the same machines with almost the same technical characteristics. The only difference that I managed to see at the exhibition at the last session of NATA in Lisbon in the spring of 2018 is to reduce the number of operating modes in Catsmart to 3 s 11 in CATS former models. Obviously, the manufacturer decided to simplify the car. It is justified or not, the future will show. In any case, the quality of reinfuzate did not deteriorate significantly [11, 12].
The principal device of most modern sellers is schematically represented in Fig. 1 and not much different from various manufacturers.
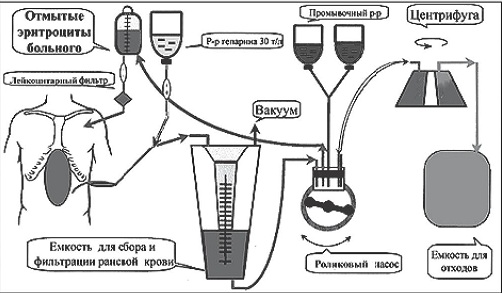
Rice. one. Circuit diagram of the device of the Sell-Seiver [14]
The main components of any sell-seater are: 1) a discontinuous two-dimensional line and a cardiotomy tank; 2) centrifuge with highways; 3) roller pump (pumps), which ensures the movement of all fluids in the sell-seater circuit; 4) Capacity for collecting washed red blood cells.
The suction line of the cell-saver differs from that of conventional surgical suction by the presence of a special second channel through which a sterile anticoagulant solution (heparin or citrate) is supplied to the suction tip.
This is important to prevent the formation of blood clots and clots in the collected wound blood. The amount of vacuum in the suction system can be important. Too high vacuum values (more than 100 cm H2O) can lead to an increase in the number of destroyed erythrocytes [8]. The cardiotomy reservoir in most commercially available cell saver models has a volume of 2-3 liters, and the built-in coarse filters allow you to remove large particles.
The centrifuge with lines is the "heart" of any cell saver. The conventional Latham type centrifuge has a distinctive bell appearance. This model, with minor modifications, is used in most cell savers manufactured by various companies. The centrifuge of the Baylor type differs slightly from it. And only in the CATS apparatus developed by Fresenius, the centrifuge is arranged in a fundamentally different way, which, unlike all other devices, allows continuous processing of wound blood [8, 13].
Roller pumps move stabilized wound blood, lavage fluid and ready-made reinfusate along the lines. The quality of reinfusate processing (Hb content) and the ingress of air emboli into the lines are controlled by special sensors of the device. The container for collecting washed erythrocytes is the last mandatory component of the cell saver before returning the reinfusate to the patient.
Processing modes
Processing modes can be different, and from this point of view, all currently available cell savers can be divided as follows:
- Treatment of wound blood is carried out discretely or continuously (it matters for the time of the procedure and the quality of the reinfusate). Continuous processing is only possible in the machine
- Possibility of manual regulation of the cleaning process. This option is available in many machines, but in CATS the process is fully automated and there is no manual process control mode.
- Actually different modes of reinfusate processing. It is believed that the number of washing cycles of the reinfusate determines its purity and, accordingly, its quality. According to the number of washing cycles, normal (five washing cycles) and high-quality (seven cycles) modes are distinguished. In the CATS cell saver, these are Quality and High Quality, respectively.
- Pediatric mode primarily provides for the possibility of working with small volumes of shed blood. This mode is not available in all machines and usually requires the use of special low volume pediatric centrifuges. In CATS, a conventional centrifuge can be used to implement the pediatric regimen, allowing you to start work with minimal volumes of blood spilled.
- The total number of processing modes. In this aspect, the undisputed "sales leader" are old models there were eleven! However, in its latest development (CatSmart), manufacturers have shifted towards simplifying software, leaving only the three most frequently used modes. In general, the comparative characteristics of the main available commercially currently, Sell-Selers are presented in the special chapter of our book [14].
The presence of a sufficient number of sellers with various technical specifications is, in our opinion, a positive point, as it allows the user to choose a car under its specific needs.
Indications and contraindications for reinfusion of blood in surgery
Under this section, it was expected to be fundamental changes over the past six years. The former, pronounced practice, the provisions remain relevant. Indications for the use of the Republic of Kazakhstan in surgery are quite simple and quite obvious: all operational interventions, which are carried out with the risk of developing massive operating blood loss. The estimated volume of the operational blood loss is, undoubtedly, an important practical factor, since, on the one hand, the Republic of Kazakhstan is a relatively notable procedure, and on the other hand, in the massive and supermassive operating blood loss, the Republic of Kazakhstan can strongly change the structure of ITT in the direction of autobrov [15]. Currently in our clinic (Neurosurgery Center. N.N. Burdenko), if for any technical reasons we cannot provide the PC to the patient with the predicted massive blood loss (1 due bcc and more), we postpone the scheduled neurosurgical intervention [sixteen].
However, there is a question of predicting the volume of the upcoming operating blood loss. For patients with neurosurgical pathology with which we are in our clinic, we managed to develop a list of such prognostic signs over the years of work (Table 1). Obviously, for any of the areas of surgery, where the application of the Republic of Kazakhstan is planned, it is necessary to formulate its similar list of prognostic criteria.
Table 1. Prognostic criteria for massive operational blood loss in neurosurgery (cyt. By [17])
Criterion
Large tumor volume and its immediate proximity to large arterial and venous manifolds
Pronounced accumulation of contrast agent tumor tumor with CT and MRI
Pronounced Own Vascular Tumor Network Contrasting under Cerebral Angiography
Anamnesis of previous surgical interventions, indicating a massive operating blood loss
Congenital or acquired hemostasis disorders in the form of hypocoagulation
Of course, like any prediction, a list of table. 1 may give an error.Но в этом случае мы рискуем лишь затратами на инсталлированный, но не использованный по назначению стартовый набор «расходки» (отсос и кардиотомный резервуар), стоимость которых невелика. Существенно же более дорогую центрифугу и магистрали следует инсталлировать уже только по факту состоявшейся массивной кровопотери [8].
По сравнению с простыми и понятными показаниями для РК в хирургии противопоказания для ее применения существенно более многочисленны и сложны. Согласно консенсусу экспертов американской ассоциации банков крови (ААВВ), противопоказания для применения РК в хирургии могут быть абсолютными и относительными [18] (табл. 2).
Table 2. Противопоказания для применения методики РК в хирургии
I. Абсолютные противопоказания
1. Наличие в раневой крови гноя
2. Наличие в раневой крови примеси содержимого толстого кишечника
3. Наличие в раневой крови примесей веществ, запрещенных к в/в введению. (некоторые антибиотики, бетадин, перекись водорода, дистиллированная вода, спирт, авитен и другие местные гемостатические препараты, созданные на основе коллагена)
II. Relative contraindications
1. Примесь в раневой крови амниотической жидкости
2. Примесь в раневой крови содержимого тонкого кишечника
3. Применение АР при онкохирургических вмешательствах
Некоторые из положений, приведенных в табл. 2, представляются нам далеко не бесспорными. Например, примесь перекиси водорода или дистиллированной воды. Понятно, что попадание этих химических соединений в кровь может спровоцировать гемолиз. Но этот процесс развивается в ране и в кардиотомном резервуаре; в дальнейшем и гемолизированные эритроциты, и свободный гемоглобин будут удалены в процессе обработки раневой крови на селл-сейвере. А наличие спирта в крови вообще не всегда омрачает жизнь! Относительные же противопоказания, как нам представляется, в настоящее время вообще перестали быть противопоказаниями.
Примесь амниотической жидкости в реинфузате. Амниотическая жидкость содержит колоссальное количество самых различных биологически высоко активных веществ, и чем обычно заканчивается ее попадание в системный кровоток матери, хорошо известно. Это тяжелейшая катастрофа с высокой летальностью. Однако есть отдельные исследования, правда только с одной из машин (CATS), в которых было убедительно показано, что при использовании режима высококачественной обработки (High Quality Wash) достижимо полное устранение амниотической жидкости из реинфузата [19, 20]. Это означает, что при использовании машин высокого класса и в режимах усиленного отмывания мы не подвергаем наших пациентов никакому дополнительному риску. Ситуация с примесью в реинфузате содержимого тонкого кишечника примерно такая же, как и в случае с амниотической жидкостью. Качественная обработка на хорошем приборе позволяет решить и эту проблему — получить качественно отмытые аутоэритроциты [8].
Oncology
This is one of the most complex and still discussed topics regarding the Republic of Kazakhstan. Let's consider it in more detail. On the one hand, oncosurgery is one of the most "bloody". Blood loss during oncosurgical interventions can often reach 2–3 volumes of the proper BCC, especially in case of multiorgan lesions or when great vessels are involved in the oncological process [21, 22]. On the other hand, the risk of viable tumor cells getting into the reinfusate and, as a result, into the patient's systemic circulation is absolutely real, and experimental studies on laboratory animals have confirmed the ability of these tumor cells to induce the growth of secondary metastatic tumor nodes [22–25]. Of course, in fairness it should be recognized that the presence of tumor cells in the patient's blood is not a phenomenon identical to metastasis. Thus, the phenomenon of the presence of tumor cells in the blood has been described in 70% of patients with gastric cancer and 50% of patients with breast cancer [22], but the statistics of distant metastasis in these patients is significantly lower. It is clear that metastasis is a complex multicomponent biological process, but the presence of tumor cells in the blood may be its fundamental factor [26, 27].
The history of the introduction of blood reinfusion into oncosurgery is interesting. In the 80–90s of the last century, when blood RK was just beginning to be actively introduced into surgical practice, a series of studies was conducted in the United States on the use of RK using cell savers specifically in oncosurgery (removal of prostate, uterine cancer, etc.) [28 –31]. A feature of these studies was that the authors did not use any measures against contamination of the reinfusate with tumor cells! How this became possible in the presence of strict control by the FDA and other similar structures in medically advanced countries is not entirely clear, but something else is interesting for us: the authors followed the follow-up of patients in groups of auto- and donor blood, and it turned out that in groups patients with reinfusion of autologous blood, even without using any measures to purify the reinfusate from the admixture of tumor cells, the survival rate was 2-3 times higher than in the groups of patients in which donor blood was used! The authors explained this by a pronounced immunosuppressive effect of donor blood components.
However, now everything is not so hopeless, and humanity has developed several solutions to this difficult problem. Here they are.
- Refusal to use a cell saver at the main stage of tumor resection [32]. However, with highly invasive tumors, this is technically not always easy, and the main most “bloody” stage of the intervention is precisely the stage of tumor removal. This, of course, means that such an approach will also inevitably reduce the effectiveness of the RC procedure itself.
- Using filters.Tumor cells that have fallen into reinfuzate can be successfully removed from it when passing through special filters. Now special filters are being developed for this purpose, the effectiveness of which is still requireing proof. Some authors, and we are among them [15], use conventional leukocyte filters with success for this purpose [33-36]. The use of leukocyte filters makes it possible to effectively reduce the number of leukocytes (up to 10-5) compared with their content in reinfusate before filtration, but it still retains, although the minimum and theoretical, but the risk of remote metastasis.
- Blood irradiation. Probably, this approach really allows you to fully solve this clinical problem. Currently, it is proved that a single irradiation of autobrings obtained as a result of the RK, a dose of 50 Gg causes a persistent violation of mitotic activity in all cells containing the kernels [21]. On the erythrocytes, not containing the nuclei, this is irradiated by any negative effect. The situation facilitates the presence of specially designed and commercially available efficient and safe devices (including domestic), specially intended for blood irradiation. When using them, the procedure takes no more than 30-40 minutes.
The presence of not even one, and the two reliable ways to solve the problem of contamination of reinfusate with tumor cells makes it possible to generally consider the possibility of effective use of blood reinfusion in oncosurgery as a solid problem. Especially shocking for me [A.L.] sounded a performance of Dr. P. Meybohm (Germany) on the sponsorship satellite symposium in Lisbon. The speaker, not much thinking, listed the oncology among the contraindications to the blood reinfusion (?!). True, as the speaker told the speaker, his experience of clinical "reinfusiology" has only five years. Well, with numerous publications of his compatriot Professor Ernil Hanzen, he seems to be simply not familiar. Oncology is currently contraindicated for blood reinfusion. It is necessary to simply use the well-known methods of decontamination of reinfuzate, the effectiveness of which is convincingly proven.
Complications of blood reinfusion techniques
Like any technique, the Republic of Kazakhstan is inherent in certain complications, although in a huge study given by DeAndrade et al. (more than 43,000 patients), the total frequency of complications of the hardware RK turned out to be extremely low – from 0 to 0.0006% [37]. These include systemic disorders of hemostasis, hemolysis, air embolism and bacterial contamination of reinfuzate.
The development of systemic violations of hemostasis in a situation of massive operational blood loss is a completely natural phenomenon due to the simple loss of platelets and plasma hemostasis factors.If you consider the fact that the selle-sewer allows you to return the patient only the washed erythrocytes, the cause of the developing hypocoagulation becomes quite understandable. It is unlikely that it is reasonable to consider this situation with the complication of RK. The correction of hemostasis disorders using donor platelets and SPPs (donor or AUTO) seems to be an effective solution to this problem [8, 15].
Earlier, the question of the possible development of systemic guidance was discussed in the literature due to anticoagulant (heparin, citrate) used to stabilize the past blood into the blood of the patient resulting as a result of reinfusion [8]. However, the subsequent studies convincingly showed that in the process of processing the wounded blood in the Selll-Seer, there is a complete laundering of the anticoagulant, and the reinfusate itself does not cause serious disorders in the hemostasis system in the patient [38-40].
Relatively rare, but as a result of the Republic of Kazakhstan, hemolysis is possible in reinfusate with subsequent hematuria and even sharp renal damage [41-43]. Its development can be promoted by obvious factors, such as mechanical damage to erythrocytes with roller pumps, blood contact with highways of the sell-seater contour, high digits of discharge in the suction that destroys the effect of ultrasonic aspirators. An independent predisposing factor is the possible pathology of the erythrocyte membranes. It is important to remember the real possibility of the development of this complication, the risk of which is particularly increasing with supermassive blood loss (2-3 due controls), when the erythrocytes pass through the contour of the selle-seater 2-3 times, and be prepared for its treatment. The key point in the treatment of this complication and the prevention of its most severe secondary complication – the development of the OPN – are the early oblastic therapy and forced diuresis.
Aerial embolism, even with death, as complication of the Republic of Kazakhstan, although it was described in the literature [44], but it is rather historical importance, as it refers to those distant times when Sell-Sellery had a very primitive design. All modern machines for the Republic of Kazakhstan are equipped with air-envelope detection sensors, which cause an immediate stopping process when even a small amount of air in the highway [14].
The problem of the bacterial contamination of the reinfusate is still underestimated. Unfortunately, this is true for our book, where this problem is not even considered. Sorry. A number of special bacteriological research revealed a fairly consequential situation: even in such relatively "net" areas of surgery as neuro- and cardiac surgery, as well as transplantology, the frequency of bacterial contamination of reinfuzate on the basis of the results of its bacteriological crops can reach 70-80% [45-47] . The main bacteria, sowned from reinfusate in these situations, are microorganisms contained in the air of the operating room and on the skin of the patient.It is clinically important, however, it remains that the AR under such a frequency of bacterial contamination is extremely rarely accompanied by signs of sepsis or generalized infection. Within the framework of the problem under consideration, certain interest is the result of meta-analysis in the frequency of infectious complications among patients who received reinfusate or donor erythrocytes to compensate for the operating blood loss [48]. The frequency of postoperative infectious complications was significantly higher in the group of patients who received donor erythrocytes that the authors tend to explain their expressed immunosuppressive effect. Similar results were obtained recently at a large array of orthopedotramathological patients [49]. Another, quite a logical approach in solving this problem was offered by Perez-Ferrer et al. [fifty]. They were added to the irigational solution of vancomycin at a concentration of 10 μg / ml. Subsequent crops of reinfuzate in the study group remained sterile, while in the control group (without vancomycin) growth was noted in 50% of observations. Reducing the bacterial contamination of reinfuzate also contributes to the use of leukocyte filters [51].
Other complications of blood reinfusion
The ingress of cobalt and chromium particles into reinfusate is described when installing metal implants in a single observation [52]. Kim and et al. The formation of fibrin clots and erythrocyte units in reinfusion in two clinical observations was described [53], but this information is unlikely to have a serious practical importance, if leukocyte filters are used for transfusion of erythroconcentratics. Immunological modulations caused by the RK procedure should be considered, the methodology is complicated – a big question [54].
Features of the application of the Republic of Kazakhstan in various fields of surgery
This information is in more detail in our book. Here we will briefly dwell only on our own key issues.
Cardiovascular surgery is apparently the main field for using the RC methodology. The magnitude of the operating blood loss is often large enough; Not only wound, but also drainage blood in the postoperative period and the contents of the contour of the artificial blood circulation apparatus can be subjected to the hardware processing; The blood of the patient often already contains anticoagulants, which prevents the development of thrombotic complications; Breast cavity, cavity of the heart and blood vessels relative to sterile. Therefore, publications on the use of RK in cardiac surgery are many. Summary definitely testifies to the effectiveness of this approach [55-57]. And this applies not only to large cardiac surgical operations, but also minimally invasive, and their complications [58, 59].
In traumatology and orthopedics, bloodstures can also be significant in terms of volume, but the main problem specific for these patients is the risk of burning gully from bone marrow to reinfuzate and further into the patient's systemic bloodstream with the development of fat embolism syndrome.The solution to this problem is associated with the use of filters, and it is interesting that special fat filters in their "delimitizing" effect turned out to be less effective than simple leukocyte [60].
Massive blood loss in obstetrics still remains one of the leading causes of maternal mortality. Given the fact that RK is the only method of healing, the effectiveness of which increases with an increase in the volume of operating blood loss, its use in obstetrics is absolutely shown [61]. The danger represents the possibility of entering the reinfuzate of the oily water with the subsequent development of embolism syndrome by the accumulative waters. However, as already mentioned above, modern sellers make it possible to effectively dissolve red blood cells and in this clinical situation, and the economic efficiency of the RK in obstetration is currently proven with a significant blood loss [62-65].
The use of RK in oncosurgery is associated with the risk of contamination of reinfusate with tumor cells, followed by the possible development of remote metastasis. The use of leukocyte filters, especially the irradiation of the reinfusion, allows to solve this problem [17].
In neurosurgery, the implementation of the Republic of Kazakhstan may be difficult due to the problem of efficient collection of wound blood. The use of ultrasound aspirators can significantly reduce the effectiveness of the RC due to increased destruction of blood cells [16]. In the case of neuroncology, the problem of possible contamination of reinfuzate with tumor cells is also relevant (its solutions are considered above).
A large number of publications over the past five to seven years is devoted to the use of hardware RK in spinal neurosurgery and when correction of scoliosis [66-71]. All authors note the clinical efficacy of the Hardware RK under these interventions, with some discrepancies in assessing the economic efficiency of the methodology. Moreover, metastatic lesions are not excluding [72, 73].
In children's surgery, especially in children of younger age, a serious problem is a small volume of reinfusate. In this clinical situation, it is extremely difficult to do without donor components of the blood, but the Republic of Kazakhstan may reduce the forced transfusion burden on the body of the operated child [74, 75].
When transplantation of the liver, the frequency of which the world in the world reaches 25,000 per year, the hardware RC is considered as a routine procedure [76].
Conclusion
The idea of compensating for the operating bloodsture in surgical interventions by returning the reputable wounded blood to the patient operated, which arose many decades ago, passed a difficult path and is currently implemented in effective medical technology. Blood reinfusion makes it possible to significantly reduce the transfusion load on the patient with donor blood components, and in some cases, with a successful combination with other heellerizing techniques, to completely abandon the use of donor components.The method of the Republic of Kazakhstan is not only developing technically, but also gets an increasing clinical distribution. We sincerely hope that briefly given here information on the method of the Republic of Kazakhstan will help increase its interest in it and even wider clinical distribution.
Conflict of interest. The authors declare the lack of conflict of interest.
Contribution of authors. Lubninn A.Yu., Gromova V.V. – Analysis of information, writing and editing the text of the article.