Low molecular weight heparins in the modern blood coagulation control system. "Dr..ru" is a scientific and practical medical reviewed magazine for doctors, scientists and teachers of medical universities.
Low molecular weight heparins in a modern blood coagulation system
Objective: Analysis of modern principles for the use of low molecular weight heparins (NMG) in various clinical situations.
Basic provisions. The modern arsenal of anticoagulants allows the use of various preparations for the mechanism of action for the prevention and long-term therapy for thrombotic complications. In order to prolonged the prevention of thrombosis of mechanical prostheses of the heart valves, the use of vitamin K. inhibitors remains
NMGs are effective drugs for routine prevention of venous thrombosis in surgery and orthopedics, as well as for their long-term therapy. Original NMGs are preferred anticoagulants in pregnant women.
Parnaparin (Fluuxum) has the greatest average molecular weight and the highest relative antithrombin activity among NMG applicable in domestic practice. The unfractionated heparin remains an indispensable drug for the treatment of heavy thrombosis of deep veins, pulmonary artery thromboembolism, as well as to provide elecorporal blood circulation.
Conclusion. Traditionally, NMG is considered as many of the same type of interchangeable drugs. However, their relative antithrombin activity is seriously varied depending on the average molecular weight (direct dependence). The most active inhibitor of thrombin from NMG, available in domestic clinical practice, is fluux (parnaparine). The high level of safety and the effectiveness of this drug makes it expedient to its wide clinical application.
Krichevsky Lev Anatolyevich – d. N., Head of Anesthesiology and Resuscitation Department No. 4 GBUZ "GKB No. 15. O. M. Filatova DzM "; Leading Researcher FGBNU "Niior them. V. A. Neochsky "Fano. 107031, Moscow, ul. Petrovka, d. 25, p. 2. E-mail: [email protected]
Random opening of heparin by a student of the Medical Faculty of the University of John Hopkins Jebe Mictalin in 1916 left at that time almost unnoticed, but later became revolutionary. Now, at the turn of the age-old anniversary of this wonderful discovery, the problem of controlling the coagulation / anticulate blood system is becoming increasingly relevant. This is due to many factors: the presence of specific diseases associated with the occurrence of thrombosis and coagulopathy; the introduction into the practice of extensive operations in patients with severe accompanying disorders; active use of extracorporeal contours in the practice of resuscitation, nephrology, etc.d.; An increase in the population of patients with pentated arteries and / or prosthetic heart valves. The problem under consideration directly concerns the doctors of almost all specialties, but especially – cardiologists, surgeons, anesthesiologists-resuscitators. Low molecular weight heparins (NMG) firmly occupied a niche of the prevention of thrombosis in the practice of intensive therapy due to their generally accepted advantages, to the number of which include: 1) ease of destination; 2) the lack of need for laboratory monitoring in most cases; 3) relative safety [13]. The use of NMG has turned into a daily routine and often remains beyond the reflection of clinicians. At the same time, this group of drugs is not entirely homogeneous, the effectiveness of NMG is not always obvious, in addition, their "pharmacological competitors" appear, which can be routine and long and long for the prevention of thrombosis without laboratory control – the so-called new oral anticoagulants (NOCA) (NOVEL ORAL Anticoagulants – NOAC) [11]. All this causes the current idea of the role of NMG in a modern antithrombotic strategy.
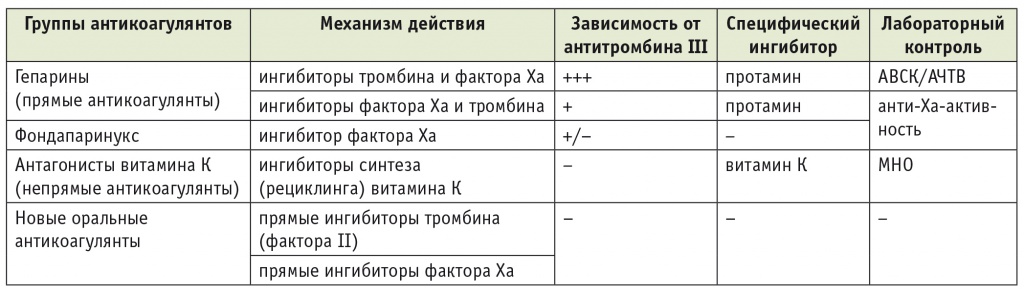
Antitrombotic drugs in a coagulative cascade. Classical ideas about the coagulation cascade as a sequence of interdependent biochemical reactions that have an external and domestic path of initiation are relevant and currently [5, 12]. If therapeutic methods of combating bleeding relatively simple and, as a rule, are to use exogenous coagulation factors in one form or other form, the mechanisms of antithrombotic therapy are presented very complex. Antitrombotic drugs directly or involving natural antithrombotic factors block various links of the coagulation cascade. Depending on the spectrum of inhibible coagulation factors, the features of the impact on them, the pharmacodynamic properties of antithrombotic drugs and the possibilities of their clinical use differ significantly. The main pharmacological groups of antithrombotic drugs are heparins (NMG and unfractionated heparin – NFG), vitamin K oral antagonists presented at present almost exclusively warfarin, as well as antitrombocytic drugs (disaggregants), the consideration of which is beyond the scope of this article. The main features of anticoagulants common in modern clinical practice are presented in Table 1.
Table 1
Pharmacodynamic and clinical features of anticoagulants common in modern clinical practice
Note. AVSK – activated blood coagulation time; ACTV – activated partial thromboplastin time; MN – international normalized attitude.
Heparins.This group of anticoagulants is customary to be called direct, in contrast to indirect anticoagulants – vitamin K inhibitors with the appearance of truly direct (immediate) inhibitors of coagulation factors from the NAK group, such terminology may seem somewhat outdated, but remains generally accepted. NFG, as is known, is a sulfur-containing glycosaminoglycan, represented by several polymer chains. The molecular weight of commercial preparations of heparin can be different, but, as a rule, hesitated within 12-16 kilodalton (kDa). The pharmacodynamic heparin profile is due to its ability to activate antithrombin III (AT-III). The most important role in this process plays a specific pentasacaride section of the heparin molecule, providing communication with AT-III. This site is available in NMG molecules and in fact in an independent form represents the drug Fondaparinux [7]. The complex "NFG + AT-III" inhibits thrombin (factor II) and activated factor Xa, as well as factors IX, XI, XII. But it is the AT-III-dependent impact on the second and tenth factors most importantly in the clinical use of heparin. Moreover, if the inhibition of the Factor XA is carried out when it is in contact with activated (any of the heparins or Fondaparinux) AT-III, then thrombin can be inhibited only by simultaneously contact with AT-III and with a polymer heparin chain. In this regard, the size of the heparin molecule determines its ability to effectively block thrombin. Accordingly, this ability is the main for NFG, less pronounced in NMG and is absent from the Fondaparinux, while inhibiting the Factor Xa is equally inherent in all the above drugs. Therefore, such "temporary" indicators, like AUSK and APTTV, informative only to control therapy of the NFG [5].
The creation of fractionated, or low molecular weight, heparins made it possible to the more convenient and safe use of direct anticoagulants. These drugs are guaranteed to be absorbed at subcutaneous administration. Due to their weakened or practically absent influence on blood throat when the NMG is destined, it is quite rare. In many clinical situations, NMG do not require laboratory control. It is quite natural that these drugs firmly occupied a niche routine prevention of thrombosis in a variety of categories of patients, primarily surgical, orthopedic patients and patients in resuscitation departments. We also emphasize the comparative safety of the long-term use of NMG in pregnant women. All this led to a rather formal, simplified attitude of clinicians to NMG as a homogeneous group of pharmacological funds, which are good for routine prevention of thrombosis, but are not sufficiently effective for the treatment of serious thrombotic complications. However, the real situation is not quite so.The scatter of the molecular weight of NMG is large enough – from 3 to 7 kDa. In turn, the molecular weight (or the length of the heparin chain) determines the severity of the inhibitory effect of the drug on thrombin. Since anti-XA activity is a stable property of all NMG, the different severity of the inhibition of thrombin is expressed as an anti-XA / anti-IIA ratio. What it is less, the antitrombic activity is higher (Table 2).
table 2
Molecular weight and relative antithrombic activity of low molecular weight heparins

As can be seen from Table 2, the direct dependence of the NMG antithrombin activity is confirmed from its molecular weight. The highest ratio of anti-XA / anti-IIA (the smallest antithrombin activity) has a drug with the smallest molecular weight (bugarine). The most "heavy" NMG, TINZAPARIN, is naturally characterized by the smallest attitude of anti-XA / Anti-IIA. From drugs available in the domestic drug market, Parnaparin (FluxSums, Alpha Wassermann, Italy) has the greatest antithrombin activity, which are used in Western Europe [6, 8, 9]. Some researchers offer to distinguish three groups of heparins on their antithrombin activity: the most active inhibitor of factor IIA – NFG; The active inhibitors of thrombin from the NMG group with a high molecular weight (Dalte-, adhesive and parnaparine – fluctuations) and, finally, the weak inhibitors of factor IIA, such as ENOCAPARIAN and NAPROPARIN [6]. The direct antagonist of all heparins is Protamin, which comes into the reaction of precipitation. The neutralization efficiency directly depends on the length of the molecular heparin chain, so the NFH is neutralized by protamine to the full extent, while NMG is only partially.
A fundamentally different mechanism of anticoagulation is characterized by vitamin K antagonists. These drugs (almost only warfarine are used) suppress the synthesis of the specified vitamin (more precisely, its recycling), thus blocking the formation in the liver of a number of coagulation factors [4, 11]. Despite the indirect mechanism, the delayed start and end of action, Warfarin remains an indispensable anticoagulant in a number of situations, primarily in patients with mechanical prostheses of the heart valves. This niche remains inaccessible for drugs from a group of NAK, which are direct, independent of the AT-III, inhibitors of the tenth factor or thrombin.
Thus, the features of the mechanism of action of a particular anticoagulant determine the expediency of its use in various clinical situations. Consider the possibility of effective and differentiated use of the traditional group of drugs – NMG.
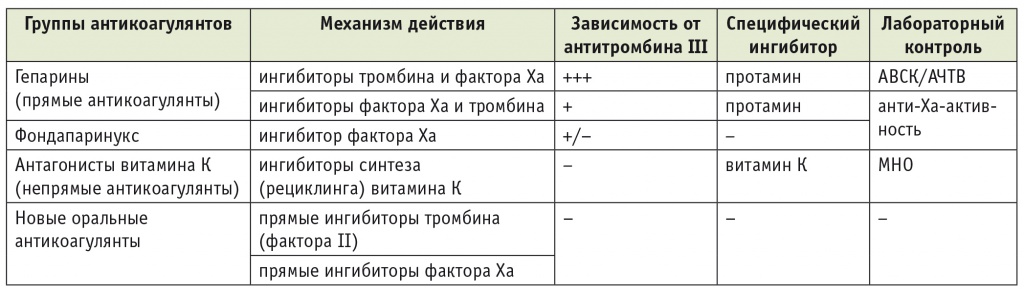
Features of laboratory monitoring with the treatment of low molecular weight heparins. Such traditional "temporary" laboratory indicators, like AUSK or APTTV, used to control the dosage of the NFG, are not applicable if NMG is appointed.Как правило, это обстоятельство не имеет отрицательного значения, так как терапия НМГ не требует никакого лабораторного контроля. Однако в ряде случаев бесконтрольное (или «стандартное») назначение НМГ является опасным. К ним относятся почечная недостаточность, масса тела менее 50 или более 100 кг, заболевания системы гемостаза, возникновение кровотечений или тромбозов на фоне антикоагулянтной терапии, в некоторых случаях — беременность. Практически единственным информативным лабораторным параметром, характеризующим эффективность НМГ, является анти-Xа-активность, выражаемая в международных единицах на мл (МЕ/мл). Имеющиеся способы оценки этого показателя достаточно дороги и сложны. Их принцип — определение активности остаточного фактора Xа после добавления в контрольный реагент, содержащий десятый фактор и избыточное количество АТ-III, плазмы больного, получающего НМГ. Чем выше остаточная активность фактора X, тем менее выражено действие НМГ. В общем виде терапия НМГ под контролем анти-Xа-активности описана в таблице 3 .
Таблица 3
Контроль анти-Xа-активности при терапии низкомолекулярными гепаринами [3]
При этом нельзя уравнивать антитромботическую активность при терапии различными НМГ и одинаковом уровне анти-Xа-активности. Необходимо учитывать, что гепарины с низкой молекулярной массой в значительной степени (а фондапаринукс — полностью) лишены ингибирующего влияния на тромбин, тогда как препараты с массой от 5 кДа проявляют отчетливый эффект в отношении второго фактора. Эта фармакодинамическая особенность никак не отражается на рекомендованном при терапии НМГ показателе — анти-Xа-активности [4] .
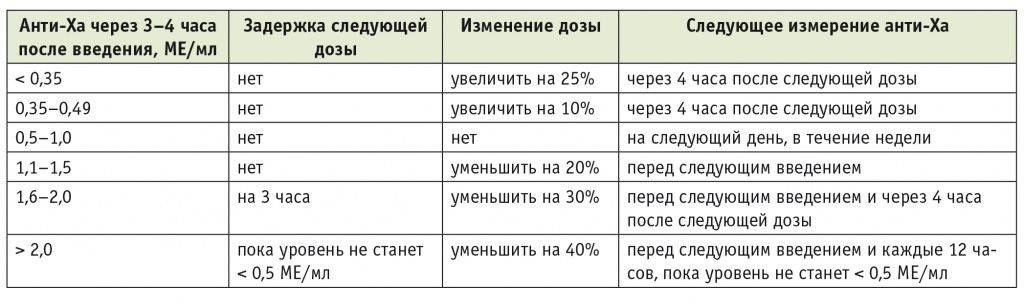
Профилактика венозных тромбозов в хирургии и ортопедии. Рутинная профилактика тромбозов глубоких вен в полостной хирургии и при ортопедических вмешательствах традиционно включает использование компрессионных средств (белья) и таких антикоагулянтов, как НФГ (сейчас крайне редко), НМГ, фондапаринукс, а в последнее время предусматривает и применение средств из группы НОАК. Антитромбоцитарные препараты в данной клинической ситуации неэффективны и достаточно опасны в связи с риском периоперационных кровотечений. Сравнение НОАК и НМГ в общем указывает на возможность эффективного профилактического применения лекарственных средств обеих групп. Однако при этом НМГ обычно рассматривают как однородную группу антикоагулянтов. Вместе с тем ранее было показано преимущество НМГ с большой (≥ 5 кДа) молекулярной массой, в частности парнапарина. Еще в 2007 г. группа итальянских авторов опубликовала впечатляющие результаты профилактического использования препарата Флюксум при артроскопии коленного сустава: дуплексное исследование не выявило ни одного (!) тромботического осложнения в группе более чем из пятисот больных ( табл. 4 ) [9] . При этом и риск кровотечений при профилактическом назначении парнапарина остается весьма низким [9] .
Table 4.
Результаты применения низкомолекулярных гепаринов
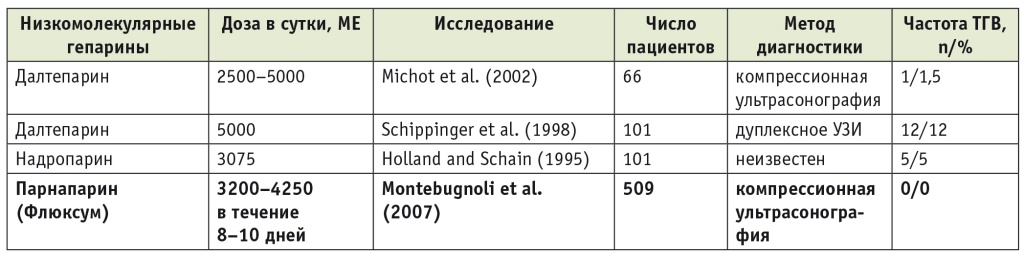
Note.TGV – Thrombosis of deep veins.
Prevention of thrombotic complications in pregnant women. Various forms of thrombophlebitis and other venous thrombosis options, unfortunately, remain very common during pregnancy. This is facilitated by the features of the hemostasis system in pregnant women [1, 2, 10] and the compression of the lower hollow vein at the later dates. The current trend of the prevention and treatment of thrombosis in pregnant women consists in determining the risk factors for thrombosis and rather aggressive and early use of NMG [8]. The authors directly prescribe to appoint NMG even with unproved suspicion of superficial thrombophlebitis and terminate this therapy only if the diagnosis is rejected after an additional examination. Moreover, on the outpatient stage of treatment, independent use of NMG is allowed. For long-term treatment of thrombophlebitis during pregnancy, NMGs are more preferable than drugs from the NAK group (warfarin and its analogs are prohibited). Of course, the ineffectiveness of NMG or the presence of thromboembolic complications (pulmony artery thromboembolism) is forced to apply a constant intravenous infusion of NFG with a target double increase in the AFTV.
An even more difficult and responsible task is to maintain pregnant women with mechanical prostatever of the heart valves. This problem can be formulated by two provisions: 1) Anticoagulant anticoagulant for prevention of prosthetic thrombosis are contraindicated in long periods of pregnancy; 2) Recommended (safe) during pregnancy anticoagulants are ineffective for the prevention of thrombosis of the mechanical prostheses of the heart valves. The authors of one of the newest publications with bitterness are: "The dilemma for the choice of anticoagulant therapy in pregnant women with [mechanical] protesters of the heart valves is still not permitted" [1]. Indeed, vitamin K antagonists (warfarin et al.) Are the most effective means of preventing prosthetic thrombosis and at the same time – powerful teratogenic agents. Their use is extremely dangerous in the first trimester. NFH, the second for preventive efficacy drug can be used, but it should be administered only as a constant intravenous infusion with the target twice increase in the AFTV. Is it possible for continuous treatment for many months? In addition, it can lead to the depletion of reserves of its own AT-III and the need for appropriate substitution therapy. Various NMGs (preferably original drugs, not their bioanalogs) in the aggregate – the third effectiveness in this clinical situation, a group of anticoagulants, their appointment is still acceptable. We emphasize that the use of NMG to prevent thrombosis of mechanical prostheses of the heart valves outside of pregnancy is completely unnecessar, and during pregnancy requires strictest laboratory control.At the same time, it should be clearly understood that LMWH is a forced, but not a full-fledged alternative to warfarin. Currently, there are no comparative studies on the use of different LMWHs in this situation. However, the above principles of their pharmacodynamics suggest that the choice of drugs with a higher molecular weight may be more reasonable. LMWHs such as parnaparin (Fluxum) combine the possibility of long-term subcutaneous use and relatively high antithrombin activity [6, 8] .
Let us consider the described clinical situation in more detail (Table 5). The first trimester of pregnancy is the most difficult for the selection of anticoagulant therapy, since during this period the laying of the organs and systems of the fetus occurs, the teratogenic effect of warfarin is most pronounced. However, it has been established that this adverse effect is characterized by a clear dose-dependence: an anticoagulant dosage up to 5 mg/day can be relatively safe [10] . American guidelines require that the risks and benefits of prescribing warfarin (no more than 5 mg/day) in the first trimester be discussed in detail with a pregnant woman who may refuse such therapy. In the event that warfarin intake is insufficient (INR less than the target value) or impossible (due to the woman's refusal), one of the heparins should be prescribed, as indicated in table 5. The period from the beginning of the second trimester to the 36th week usually does not present any difficulties, since taking warfarin at the required dosage is quite acceptable. An additional prescription of aspirin at a dose of 75–100 mg/day is also recommended. Further, only intravenous infusion of UFH is prescribed with a target two-fold rise in APTT, which is stopped 4-6 hours before, and resumed 4-6 hours after delivery [10] .
Table 5
Prevention of thrombosis of mechanical prosthetic heart valves during pregnancy
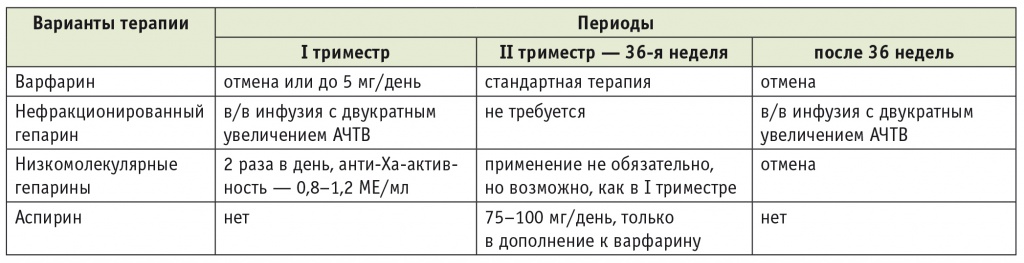
Note. APTT – activated partial thromboplastin time.
Thus, LMWH firmly occupy their niche in the general spectrum of anticoagulant drugs, primarily in the prevention of thrombotic complications, the treatment of various forms of thrombophlebitis, and, of course, in pregnant women. The pharmacological group of LMWH is not homogeneous. The most important distinguishing property of drugs is their antithrombin activity, which directly depends on the molecular weight and is inversely expressed by the value of anti-Xa / anti-IIa.
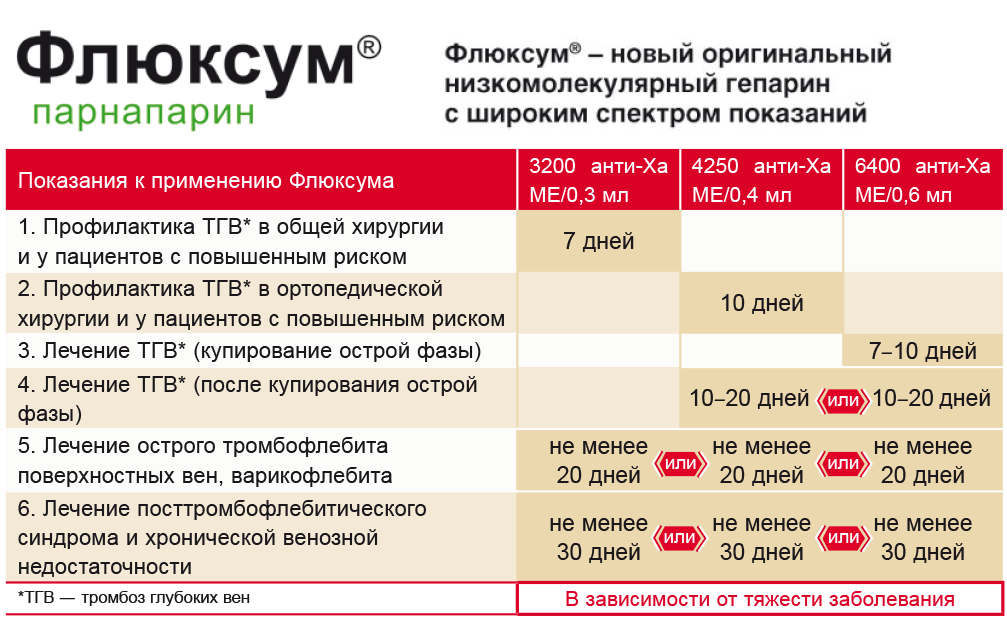
Parnaparin (Fluxum) is a new low molecular weight heparin in Russian practice. We consider it appropriate to draw the attention of readers to the fact that an original LMWH from Italy, parnaparin (Fluxum), has appeared in Russia. This drug differs from nadroparin, enoxaparin, etc., traditionally used in routine practice, by a relatively large molecular weight (5 kDa), which means a relatively high antithrombin activity.In this regard, Fluxum is not only more effective when prescribed according to traditional indications for LMWH, but also has some of its own indications, which are absent in other LMWHs, such as post-thrombophlebitic syndrome. In terms of its characteristics, parnaparin approaches the drug dalteparin, which is better known to Russian colleagues, but the ratio of anti-Xa / anti-IIa in parnaparin is somewhat lower (see Table 2). At the same time, parnaparin is characterized by high safety and the possibility of long-term outpatient use. It is important that the drug is produced in different dosages: 3200 anti-Xa IU (0.3 ml), 4250 anti-Xa IU (0.4 ml) and 6400 anti-Xa IU (0.6 ml). The doses of parnaparin and the frequency of its administration (1 or 2 times a day) differ depending on the goals of therapy (prevention or treatment) and the clinical situation (Fig. ) [6, 8, 9] .
Rice. The tactics of using the drug parnaparin (Fluxum)
Despite the creation of more and more new drugs for anticoagulant therapy, low molecular weight heparins (LMWHs) remain the drugs of choice for routine prevention and long-term treatment of thrombosis. It is this group of anticoagulants that is preferable in such a complex category of patients as pregnant women. Traditionally, LMWHs are considered as a set of the same type of interchangeable drugs. However, their relative antithrombin activity varies greatly depending on the average molecular weight (direct relationship). The most active thrombin inhibitor among LMWHs available in domestic clinical practice is parnaparin (Fluxum). The high level of safety and efficacy of this drug makes it reasonable for its widespread clinical use.